Micro Medical provides practical solutions to support practice efficiency through advanced portable technology.
VF2000 VISION DIAGNOSTIC PLATFORM
Modernize Your Practice with a Portable Vision Diagnostic Platform
The VF2000 platform helps your practice perform visual field and specialty vision testing with a compact VR headset designed to save space, improve patient comfort, and modernize the clinical experience.
SCHEDULE A DEMO30-DAY TRIAL
No deposit. No commitment fee. Try it with your own patients and staff.

Portable
Scalable
Practical
Portable, Scalable, Practical
30
+
Visual Field Patterns
1,550
+
Offices World Wide
650
K+
Patients Tested
1.4
M+
Reports Generated

VF2000-NEO
The VF2000-NEO takes the versatility of the VF2000-G2 and pairs it with our newest innovation, Active Eye Tracking. Active Eye tracking follows the gaze of patients during a visual field test, allowing for more precision in this important test.
Improve Your Clinical Practice with Micro Medical
When you’re ready to learn more about how Micro Medical products can help you increase the efficiency and diagnostic accuracy of your clinical practice, give us your information and we’ll be in touch shortly.

VF2000-G2
The VF2000-G2 is the perfect option for practices looking to incorporate virtual reality on a deeper level. Equipped with an upgraded 4K display, the VF2000-G2 adds the capability to perform a range of visual screening tests in addition to its visual field capability.

PALMSCAN-PRO
Our most versatile and adaptable solution, the PalmScan Pro available for our full suite of biometry tools.

A-SCAN BIOMETERS
MMD A-Scan devices use ultrasound technology to precisely measure axial length, lens thickness, and anterior chamber depth, for cataract surgery and myopia management.
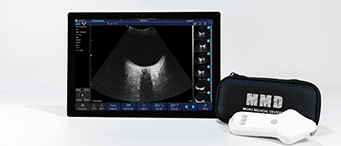
iVIEW B-SCAN
The new iView B-Scan replaces our classic Mobile B-Scan with a wireless, solid-state probe with no moving parts, high-resolution imaging system designed for speed, reliability, and portability.

AUTO KERATOMETER
The MMD Auto Keratometer device is handheld, USB-based technology that measures the outer curvature of the eye to assist in planning for a lens replacement procedure.

PACHYMETERS
MMD’s Pachymeter devices measure corneal thickness to help detect a range of eye conditions. They’re capable of measuring extremely thin corneal grafts (under 100 micron).

Corneal Crosslinking enables doctors to slow the progression of keratoconus in their patients. The MMD OMNI system provides focused UV light, critical for effective treatment.
Meet the VF2000
Aware of how much of a bottleneck traditional Visual Field Analyzers can be to the ongoing development and growth of the practice, we developed the VF2000 with the everyday doctor in mind. Able to run threshold, neuro, and ptosis tests in perfect alignment with the Humphrey Field Analyzer and generate familiar, easy to read reports, this innovation is a must have for the modern practice.
Why Choose Us
Innovative Eyecare Solutions That Drive Practice Growth
At Micro Medical Devices, we’ve spent over two decades redefining what’s possible in ophthalmic diagnostics. Our mission is simple: deliver portable, scalable, and practical technologies that empower eye care professionals to work more efficiently—without compromising accuracy or patient care.
A Portfolio Built for Performance
From the pioneering VF2000 series with Active Eye Tracking to our ultrasound-based A and B Scans, Pachymeters, and Auto Keratometers, every device is built to enhance clinical workflows and integrate seamlessly into your existing operations.
Proven Technology, Trusted Results
With 20 years of clinical success, our solutions are engineered for the real-world demands of modern practices. Whether you’re managing patient flow, adding new services, or improving diagnostic confidence, our tools are designed to grow with you.
To learn more about how Micro Medical products can help you increase the efficiency and diagnostic accuracy of your clinical practice, give us your information, and we’ll be in touch shortly.
Why Choose Our Visual Field Analyzers
Micro Medical Devices is a technology company that specializes in developing portable, handheld technology to help solve day-to-day challenges for a new generation of eye care practitioners. We’re led by a team of engineers, designers, and clinical experts, committed to combining our expertise for the benefit of the people who use our products.
TESTIMONIALSMEET OUR LEADERSCOMMITMENT TO
YOUR SUCCESS
Micro Medical Devices has taken great pride in delivering complete solutions to practices. Our solutions don’t stop at just innovative technologies. Every product is backed by our unconditional 100% satisfaction guarantee. Our team of committed practice advocates are available live to ensure that your practice gets maximum value from your MMD product.
Want to try a product in your practice?

Trusted by Eye Care Professionals Around the Globe
At MMD, we’re proud to support humanitarian organizations delivering vital eyecare to underserved communities worldwide. Our PalmScan portable ophthalmic ultrasound biometers are used by U.S.-based outreach groups in global missions, helping improve vision and quality of life in areas with limited access to advanced medical technology. Together, we’re making a meaningful difference—one patient, one mission at a time.
Testimonials
Frequently asked questions
What products does Micro Medical Devices offer?
MMD offers a full range of portable ophthalmic diagnostic tools including the VF2000-NEO and VF2000-G2 virtual reality visual field analyzers, A-Scan and iView B-Scan ultrasound biometers, the PalmScan PRO, Pachymeters, Keratometer, and the OMNI Corneal Cross-Linking System all designed for use in and out of the traditional office setting.
Are Micro Medical Devices products HIPAA compliant and certified?
Yes. All Micro Medical Devices products are HIPAA-compliant, ISO 13485 certified, ADA compliant, and manufactured in the USA. MMD also holds a 510(k) clearance. These certifications reflect MMD’s commitment to patient safety, data security, and clinical reliability across all product lines.
How many practices use Micro Medical Devices equipment?
Micro Medical Devices equipment is currently used by more than 1,550 offices across six continents. MMD devices have been used to test over 650,000 patients and have generated more than 1.4 million reports to date, making MMD one of the most widely adopted portable ophthalmic diagnostic brands globally.
What industries and practice types does Micro Medical Devices serve?
Micro Medical Devices serves ophthalmology, optometry, neuro-ophthalmology, visual therapy, and sports vision practices of all sizes. Use cases include visual field testing, cataract surgery planning, corneal cross-linking for keratoconus, myopia management, sports vision performance assessment, and portable diagnostic screenings in humanitarian field programs.
Can I try a Micro Medical Devices product before purchasing?
Yes. MMD offers a no-obligation demo so eye care professionals can experience the devices firsthand in their own practice setting. Every product is also backed by an unconditional 100% satisfaction guarantee. To schedule a demo, Click Here.
Does the VF2000 require additional subscription fees?
No, the VF2000 does not require additional subscription fees for core operation, cloud storage access, or standard future software updates. The system is designed as an owned platform rather than a per-test or subscription-dependent ecosystem. Clinics can perform visual field testing, generate reports, utilize the web portal/cloud functionality, and benefit from ongoing software improvements without mandatory recurring licensing fees.
Ready to Streamline Your Practice?
From cutting-edge technology to hands-on practice advocacy, we’re here every step of the way.

Contact Us
Call Us
Office: 818-222-3310
Toll-Free: 866-730-0663
WhatsApp (Sales): +1 (818) 798-4569
WhatsApp (Support): +1 (747) 369-5742
Office: 818-222-3310
Toll-Free: 866-730-0663
WhatsApp (Sales): +1 (818) 798-4569
WhatsApp (Support): +1 (747) 369-5742
Micro Medical Devices
23945 Calabasas Rd, Suite 110, Calabasas, CA 91302
23945 Calabasas Rd, Suite 110, Calabasas, CA 91302
Hours
Monday-Friday: 9am-5pm PST
Saturday-Sunday: Closed
Monday-Friday: 9am-5pm PST
Saturday-Sunday: Closed



